pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed

Dong Hye Suh,Hyung Jin Park,Sang Jun Lee,Hyunjoo Kim,Ki-Heon Jeong,Mu-Hyoung Lee,Min Kyung Shin
10.17966/JMI.2019.24.1.19 Epub 2019 March 28
Abstract
Background: Laser therapy can be used as an alternative treatment for onychomycosis; however, there are some limitations to its efficacy as a single agent.
Objective: To evaluate the effectiveness of combination therapy with 1,064-nm neodymium-doped yttrium aluminum garnet (Nd:YAG) laser and topical efinaconazole in onychomycosis treatment and identify factors influencing the therapeutic outcomes of combination treatment.
Methods: Big toenails with onychomycosis were treated by 1,064-nm Nd:YAG laser at 4-week intervals with daily application of topical efinaconazole. Therapeutic response was assessed through onychomycosis severity index (OSI) and percentage of nail infected (PNI), and its association with a variety of factors that may affect treatment outcome was evaluated.
Results: One hundred big toenails were included in the study and significant clinical improvements were observed after treatment (OSI improvement score = 76.68 ± 28.83, PNI improvement score = 72.37 ± 30.37). There was no difference in treatment response according to the number of laser treatments, onychomycosis clinical type, or initial severity. However, patient age was negatively correlated with clinical improvement (p = 0.019). Also, female patients had better therapeutic responses than male patients.
Conclusion: Combined treatment with Nd:YAG laser and topical efinaconazole has a significant therapeutic effect on onychomycosis. A randomized controlled trial is warranted in the future.
Keywords
Combination treatment Laser Onychomycosis
Onychomycosis is a common nail disorder caused by a fungal infection. It is known that 2~13% of the general population is affected by onychomycosis, and the prevalence is higher in the elderly, reaching 14~28%. Although there are various treatment options for onychomycosis, oral antifungal agents such as terbinafine, itraconazole, or fluconazole are the treatments of choice. Unfortunately, these agents are contraindicated in some patients, including those with severe hepatic or renal diseases, pregnant or lactating females, and in those with hypersensitivities to these drugs. In addition, drug interactions are often a concern1. Topical antifungal agents and recently introduced laser devices are alternative therapeutic modalities for treating onychomycosis.
Various laser devices, including the neodymium-doped yttrium aluminum garnet (Nd:YAG) laser, have been developed for the treatment of onychomycosis. Although there are many reports that lasers are effective for treating nail fungal infection, other studies yielded disappointing results2-6. Further, the mycological cure rate appears relatively low7. In this context, the US Food and Drug Administration currently indicates these devices for "temporary increase in clear nails", and the devices are not considered curative, or able to eradicate pathogenic fungi. A recently published review article concluded that there was limited evidence that laser therapies eradicated pathogenic fungi in patients with onychomycosis8. Topical agents such as amorolfine, ciclopirox, and tioconazole have been used for onychomycosis treatment, but they are less-frequently recommended, and their therapeutic effects are smaller than systemic antifungals. Topical agents are recommended for superficial white onychomycosis (SWO) or distal and lateral subungual onychomycosis (DLSO) with nail involvement less than 50% or 80%1-9.
Because both of the above treatments have some limitations as single modalities we evaluated the possibility of a combined treatment. Although there is exists no published head-to-head comparative study, topical efinaconazole is recommended as a first-line topical treatment1 based on its superior mycological cure rates, as determined by meta-analysis. Therefore, we examined the therapeutic effects of a combination treatment consisting of 1,064-nm Nd:YAG laser (which shows a high clinical clearance rate) and topical efinaconazole solution (with a better mycological cure rate).
There are two previous studies of treatments that combined lasers and topical antifungals10,11, but the number of laser treatments was restricted and factors associated with therapeutic responses were not analyzed. In this study we observed patients' therapeutic responses following combined treatment and analyzed the factors that potentially affected treatment efficacy.
This study was approved by the hospital's Institutional Review Board (KHUHMDIRB 2018-10-064) and conducted according to principles of the Declaration of Helsinki. A retrospective chart review was conducted wherein data were collected for patients with onychomycosis who were treated using a combination therapy consisting of a 1,064-nm Nd:YAG laser and topical efinaconazole, between July 2017 and September 2018. We also searched for any recorded adverse events that occurred during or after treatment.
1. Patients
Patients with clinical features of onychomycosis on their big toenails, confirmed by mycological evaluation were enrolled. Mycological diagnosis of onychomycosis was based on microscopic examination after treatment with 20% potassium hydroxide (KOH). In cases of ambiguous results upon microscopic examination, a fungal culture on Sabouraud's dextrose agar with incubation at room temperature (25~27℃) for up to 4-weeks was performed. Patients taking oral antifungal medications within 6-months of the study and those using other topical antifungal agents, other than the topical solution of 10% efinaconazole, within 1-year of the study were excluded. We excluded patients with permanent discoloration of the nail plate and those with concomitant nail diseases, such as nail psoriasis.
2. Treatment protocol
Before treatment, photographs were taken in a standardized format using a digital camera (Canon EOS-40D; Canon Corp., Tokyo, Japan). If the target toenail was thicker than 2 mm, it was mechanically debrided using a nail grinder before the laser treatment. All patients were treated using a 1,064-nm Nd: YAG laser (PinpointeTM FootlaserTM; Pinpointe USA Inc., Chico, CA, USA) at the following settings: pulse energy, 200 mJ; pulse width, 0.1 ms; spot size, 1.5 mm; frequency; 30 Hz. The laser beam was moved in a spiral fashion to cover the entire nail plate. This procedure was repeated twice with a 2-minute pause between treatments. Laser treatments were scheduled at 4-week intervals (±2 weeks). Throughout this time, all subjects were educated to self-apply a topical solution with efinaconazole 10% to their infected big toenails once daily. If 100% clinical clearance was observed, treatment was paused and a final follow-up evaluation was scheduled 4-weeks later.
3. Outcome assessment
Clinical improvement was evaluated using the onychomycosis severity index (OSI)12 and percentage of nail infected (PNI). For OSI, the degree of involvement was scored as follows: 0, 0% invasion of the entire nail surface from onychomycosis; 1, invasion ratio 1 to 10%; 2, invasion ratio 11 to 25%; 3, invasion ratio 26 to 50%; 4, invasion ratio 51 to 75%; and 5, invasion ratio 76 to 100%. In addition, the nail from the edge to the proximal nail fold was divided into four sections and invasion was scored as follows: 1, 1/4 or less; 2, 1/4 to 1/2; 3, 1/2 to 3/4; 4, 3/4 or more; 5, invasion had proceeded to the nail lunula or nail matrix. To obtain the final OSI value, these two scores were multiplied and 10 points were added if we observed dermatophytoma or subungual hyperkeratosis of 2 mm or greater. OSI was evaluated by three dermatologists including the therapist, and the mean value of the three evaluations was adopted. The OSI improvement score (OIS) was defined as the difference between initial OSI and final OSI divided by initial OSI. Favorable response rate was defined as the percentage of toenails where OSI decreased by more than 75% compared to the initial value. PNI was defined as the ratio of the big toenail area showing clinical symptoms of onychomycosis, and the PNI improvement score (PIS) was calculated in the same way as OIS. The clinical cure rate was estimated as the proportion of toenails in which final OSI was less than 5, and final PNI was less than 10.
4. Statistical analysis
All statistical analyses were computed using SPSS software version 20.0 (SPSS Inc., Chicago, IL, USA) Continuous variables are presented as means ± standard deviations. We used a paired t-test to evaluate improvement in OSI and PNI pre- to post-treatment. Pearson's correlation and regression analyses were performed to study the relationship between OIS or PIS and other variables. Patients were divided into two severity groups based on the nail variables proposed by Park et al.1 and Student's t-test, analysis of covariance, and Pearson's chi-square test were used to analyze differences in treatment response. A p-value less than 0.05 was considered to reflect statistical significance.
A total of 100 infected big toenails from 86 patients were included in this study (Table 1). There were 27 patients with underlying disease (Table 2). Three patients were immunocompromized due to medication for ulcerative colitis or were in a kidney transplanted state because of chronic renal failure, or a liver transplanted state after hepatectomy because of hepatocellular carcinoma. Table 1 shows the patients' demographic data and therapeutic responses of enrolled big toenails.
|
Characteristics |
|
|
|
Patients
(nails) |
86 (100) |
|
|
Age
(years) |
51.62 ± 12.88 (11~80) |
|
|
Clinical
type |
DLSO† |
72 |
|
SWO‡ |
14 |
|
|
TDO§ |
14 |
|
|
PSO∥ |
0 |
|
|
Treatment
number |
8.38 ± 4.07 (3~16) |
|
|
Initial
OSI¶ |
13.63 ± 7.98 |
|
|
Final
OSI |
3.60 ± 5.58 |
|
|
OIS** |
76.68 ± 28.83 |
|
|
Initial
PNI†† |
49.35 ± 30.11 |
|
|
Final
PNI |
14.65 ± 20.89 |
|
|
PIS‡‡ |
72.37 ± 30.37 |
|
|
Favorable response rate*** |
68% |
|
|
Clinical cure rate**** |
64% |
|
|
Immunocompromized patients (n = 3) |
||
|
Ulcerative colitis (n
= 1) |
||
|
Kidney transplanted
state because of chronic renal failure (n = 1) |
||
|
Liver transplanted
state after hepatectomy because of hepatocellular carcinoma (n = 1) |
||
|
Immunocompetent patients (n = 24) |
||
|
Hypertension (n = 6*) |
Heart
failure (n = 1*) |
Chronic
hepatitis B carriers (n = 3*) |
|
Hyperlipidemia (n =
1) |
Stroke
(n = 1*) |
Fatty
liver (n = 2) |
|
Diabetes mellitus (n
= 4*) |
Breast
cancer (n = 1) |
Gastritis
(n = 5*) |
|
Hypothyroidism (n =
1) |
Rheumatic
arthritis (n = 1) |
Benign
prostate hyperplasia (n = 1) |
|
Meniere's disease (n
=1) |
|
|
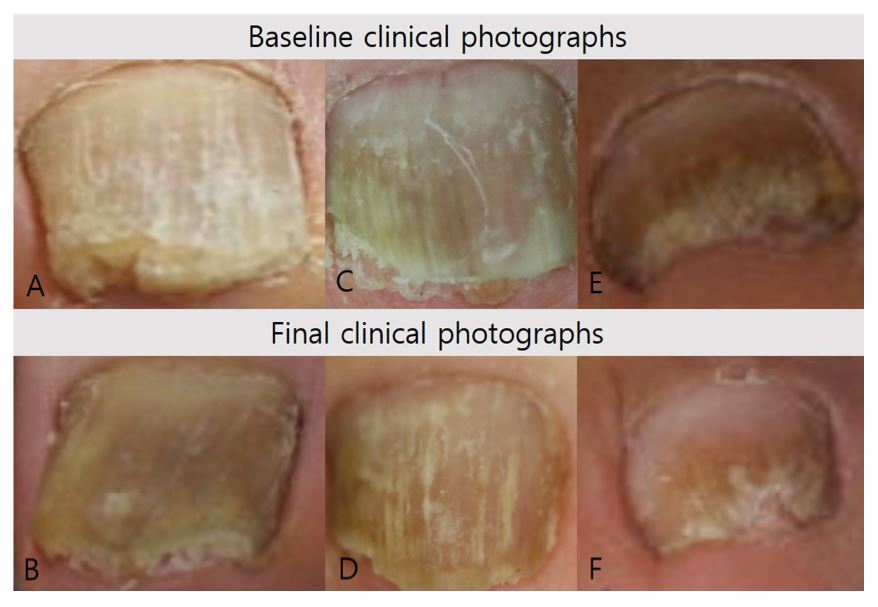
The mean age of the included patients was 51.62 ± 12.88 years, and the average number of treatments was 8.38 ± 4.07. Both OSI and PNI significantly decreased after treatment (p < 0.001 for both). OIS was 76.68 ± 28.83 and PIS was 72.37 ± 30.37. The favorable response rate was 68% and the clinical cure rate was 64% (Table 1). Figure 1 shows representative cases with favorable improvement after treatment and Figure 2 shows representative cases with no significant changes after treatment.

We considered age, the number of treatments, clinical type, and initial severity as factors that might be related to treatment response, and analyzed the relationship between these variables and OIS or PIS (Table 3). During Pearson's correlation analysis, age and clinical type showed a weak negative correlation, but no significant relationship was confirmed in the partial correlation analysis controlling for other variables. For PIS, age showed a weak negative correlation with PIS during the partial correlation analysis, and the regression equation was as follows: [PIS = 110.270 - (0.734 × age), p = 0.002, adjusted coefficient of determination = 0.087]. Clinical type was associated with PIS during Pearson's correlation analysis, but not during partial correlation analysis.
|
Correlation with OIS |
Coefficient of correlation* |
Partial correlation coefficient† |
Adjusted coefficient of |
|
Age |
-0.268 (p = 0.007) |
-0.196 (p
= 0.056) |
- |
|
Number of treatments |
0.106
(p = 0.294) |
0.029
(p = 0.776) |
- |
|
Clinical type |
-0.207 (p = 0.039) |
-0.068 (p
= 0.511) |
- |
|
Initial OSI |
-0.185 (p
= 0.065) |
-0.078 (p
= 0.450) |
- |
|
Correlation with PIS |
Coefficient of correlation* |
Partial correlation coefficient† |
Adjusted coefficient of |
|
Age |
-0.310 (p = 0.002) |
-0.238 (p = 0.019) |
0.087 (p = 0.002) |
|
Number of treatments |
0.169
(p = 0.093) |
-0.090 (p
= 0.382) |
- |
|
Clinical type |
-0.216 (p = 0.031) |
0.086
(p = 0.405) |
- |
|
Initial PSI |
-0.112 (p
= 0.267) |
0.005
(p = 0.960) |
- |
Next, we divided the patients into two groups according to the presence or absence of nail variables that reflect the severity of onychomycosis. Toenails with a SWO type or DLS type with less than 50% of area involvement were assigned to the mild onychomycosis group, and toenails showing DLSO type with an area involvement greater than 50%, TDO type, or toenails with spikes, fungal balls, dermatophytoma, or subungual hyperkeratosis thicker than 2 mm were classified as the moderate to severe onychomycosis group. We analyzed the difference in treatment response between the two groups (Table 4).
|
|
Mild onychomycosis* (n = 58) |
Moderate to severe onychomycosis† (n = 42) |
p value |
|
Age |
48.16 ± 11.87 |
56.33 ± 12.83 |
p = 0.001‡ |
|
Number of treatments |
8.56 ± 4.25 |
8.05 ± 3.86 |
p = 0.897§ |
|
OSI |
9.37 ± 5.31 → 1.60 ± 2.37 |
19.60 ± 7.21 → 6.38 ± 7.33 |
|
|
OIS |
81.95 ± 27.04 |
69.36 ± 30.22 |
p = 0.159§ |
|
PNI |
34.12 ± 19.71 → 7.02 ± 9.11 |
70.36 ± 29.66 → 25.12 ± 27.33 |
|
|
PIS |
77.45 ± 28.70 |
65.50 ± 31.91 |
p = 0.294§ |
|
Favorable response rate |
75.86% |
57.15% |
p = 0.018∥ |
|
Clinical cure rate |
81.03% |
40.48% |
p < 0.001∥ |
There was no difference in the number of treatments between the two groups, but mean age was higher in the moderate to severe onychomycosis group (p = 0.001). Because age is likely to affect treatment response (Table 3), we performed an analysis of covariance (ANCOVA), controlling for age. ANCOVA showed no between-group difference in OIS or PIS. However, both favorable response rate (p = 0.018) and clinical cure rate (p < 0.001) were higher in the mild onychomycosis group.
Finally, we studied whether the treatment response differed by sex (Table 5). Mean age (p = 0.549), number of treatments (p = 0.210), initial OSI (p = 0.439), and PIS (p = 0.905) did not differ between male and female patients, and the treatment response in females was favorable for all aspects of OIS (p = 0.017), PIS (p = 0.015), favorable response rate (p = 0.001), and clinical cure rate (p = 0.036). No patients discontinued treatment because of side effects, and no sustained side effects other than a temporary heating sensation were recorded.
|
|
Male toenail (n = 34) |
Female toenail (n = 66) |
p value |
|
Age |
52.71
± 9.70 |
51.06
± 14.30 |
p = 0.549† |
|
Number of treatments |
8.50
± 4.19 |
8.31
± 4.04 |
p = 0.210† |
|
OSI |
12.76
± 7.31 → 4.59 ± 5.93 |
14.08
± 8.32 → 3.09 ± 5.36 |
|
|
OIS |
67.19
± 31.61 |
81.56
± 26.22 |
p = 0.017† |
|
PNI |
49.85
± 30.76 → 20.29 ± 24.71 |
49.09
± 30.01 → 11.74 ± 18.16 |
|
|
PIS |
62.16
± 31.59 |
77.63
± 28.56 |
p = 0.015† |
|
Favorable response rate |
47.06% |
78.79% |
p = 0.001‡ |
|
Clinical cure rate |
50.00% |
71.21% |
p = 0.036‡ |
Laser therapies for onychomycosis have recently been in the spotlight as alternative treatment options for patients who cannot be treated with oral antifungal agents or are reluctant to undergo such treatments1. Most published studies of laser therapy for onychomycosis used 1,064-nm Nd:YAG lasers. Although many studies have reported the efficacy of 1,064-nm Nd:YAG for treating nail fungal infections, some studies showed conflicting results2-6. The therapeutic mechanism of laser therapy for onychomycosis has not yet been elucidated; however, there are several hypotheses, including local hyperthermia-induced fungal apoptosis and an indirect antifungal effect, selective photo-thermolysis targeting melanin in fungal cell walls, keratin denaturation altering the nail bed environment, and promotion of nail growth due to thermal effects2,3,13,14. Another problem with this therapy is that the mycological cure rate is lower than the clinical cure rate7.
Topical antifungal agents are an alternative treatment option in patients with contraindications for systemic antifungals, but their therapeutic effects are often insufficient. The role of monotherapy with topical antifungals is limited by the hard keratin and compact structure of the dorsal nail plate that acts as a barrier to topical drug diffusion; further, the hydrophilic nature of the nail plate precludes absorption of these drugs9. In this regard, we investigated the efficacy of a combination treatment consisting of lasers with topical efinaconazole to improve treatment results.
There are two previous reports of combined treatments with topical antifungal agents and lasers for onychomycosis. Bonhert et al.10 conducted a 48-week clinical study with daily self-application of topical efinaconazole and 6 Nd:YAG laser treatments every 4 weeks. They reported an approximately 70% rate of clinical improvement, as evaluated by a scoring system at week 48. Park et al.11 reported that the lesion-free area increased from 40.76% to 74.39% at week 16 (which is about 48.33% in terms of PIS used in this study) after 4 sessions of Nd:YAG laser treatment with daily topical amorolfine nail lacquer application.
We found that combination therapy, with an average 8.4 sessions of 1,064-nm Nd:YAG laser treatment and daily application of topical efinaconazole for 9 months, resulted in a greater than 70% clinical improvement rate as evaluated by OSI and PNI. The favorable response and clinical cure rates were approximately 60 to 70%. Although the study design and treatment protocol were different, our results are generally consistent with those of the previous studies of combination treatment. In comparison with the treatment efficacies reported in pre-existing studies we are able to at least partially determine whether the combination therapy has a superior effect over monotherapy (laser or topical medication).
For topical efinaconazole, Pollak et al.15 reported that at week 48, 39.1% of participants achieved treatment success, defined as at least a 50% improvement in affected toenails from baseline. The median PNI decreased from 50% to 40%. Elewski et al.16 reported that treatment success (defined as percent affected target toenail ≤ 10%) for efinaconazole ranged from 17.9% to 44.8% at week 48. For laser treatment, Kim et al.2 showed that at weeks 12, 25.3% of patients, and at week 24, 31.6% of patients showed marked improvement, defined as greater than 75% increase in normal appearing nail length. Yang et al.17 reported that the clinical clearance rate was 29.03% at week 12 and 64.52% at week 24. Therefore, it can be inferred that the combination treatment used in this trial produces superior therapeutic results than monotherapy of either laser or topical antifungals.
We also reviewed patients' ages, sex, number of treatments, onychomycosis clinical type, and initial severity as candidate factors that could affect the clinical outcomes. We found that age and sex had some impact on the outcomes. This is consistent with a report by Gupta and Paquet3, showing that patients younger than 60 years and female patients had better outcomes and that initial severity did not affect therapeutic outcomes. We hypothesized that increased nail thickness or nail surface changes, such as onychorrhexis resulting from the natural process of aging, decreases the laser beam penetration and increase scattering18. However, since the adjusted coefficient of determination in our study was low at 0.087, the effect of age was not strong. In contrast, sex-related differences in nail plate character such as thickness appear to have affected treatment response. It is also possible that female patients had higher compliance with the topical treatment than male patients. Further studies are required to identify other factors that may influence therapeutic outcomes. There was no significant difference in OIS and PIS between the mild onychomycosis group and moderate to severe onychomycosis group, as determined by nail variables that reflected severity. This result suggests that the above combination treatment might be more effective than topical antifungal treatments, even for severe cases of onychomycosis.
A strength of our study is that we obtained long-term, real-world data for up to 16 laser treatments. In previous studies of combination therapy, even though the follow-up period was up to 52 weeks, only 4~6 laser treatments were performed. In the absence of clinical improvement, we continued laser therapy, so the number of treatments in this study was higher than in previous reports. Nevertheless, there was no direct correlation between the number of treatments and clinical improvement. It can be hypothesized that if only a certain number of laser treatments are given, the number of sessions does not have a decisive influence on therapeutic outcomes. However, further research is needed to verify this hypothesis. In addition, we cannot exclude the possibility that improved clinical outcomes, according to the number of treatments, are masked by the present study design which was based on clinical data. Notably, treatments are likely to be discontinued, when clinical improvement is observed. Because the growth rate of the big toenail is faster than those of other nails, and the involved area was easier to determine, the results of this study are likely to be more consistent than those of other studies that included all nails. In addition, the effectiveness of our treatment was verified using multiple scoring systems.
Several study limitations should be noted and considered. A follow-up mycological study was not performed and, as a consequence, we could not evaluate the mycological cure rate. In addition, differences in outcomes according to mycological species were not determined. Further research is needed, including a prospective randomized controlled study to overcome these limitations.
In conclusion, we show that 1,064-nm Nd:YAG laser treatment combined with topical efinaconazole solution application significantly improved onychomycosis symptoms and possessed a good safety profile. Observed treatment effects appeared to be independent of initial severity. However, the treatment effect may be somewhat reduced as patient age increases and better therapeutic effects were observed in female patients.
References
1. Park J, Nam JH, Lee JH, Park JS, Mun JH, Lee YW, et al. Korean guideline for the diagnosis and treatment of onychomycosis: purpose and process of algorithm guide- line development. J Mycol Infect 2018;23:33-44
Crossref
Google Scholar
2. Kim TI, Shin MK, Jeong KH, Suh DH, Lee SJ, Oh IH, et al. A randomised comparative study of 1,064 nm Neodymium-doped yttrium aluminum garnet (Nd:YAG) laser and topical antifungal treatment of onychomycosis. Mycoses 2016;59:803-810
Crossref
Google Scholar
3. Gupta AK, Paquet M. A retrospective chart review of the clinical efficacy of Nd:YAG 1,064-nm laser for toenail onychomycosis. J Dermatolog Treat 2015;26:376-378
Crossref
Google Scholar
4. Wanitphakdeedecha R, Thanomkitti K, Bunyaratavej S, Manuskiatti W. Efficacy and safety of 1,064-nm Nd:YAG laser in treatment of onychomycosis. J Dermatolog Treat 2016;27:75-79
Crossref
Google Scholar
PubMed
5. Kim MS, Jung JY, Cho EB, Park EJ, Kim KH, Kim KJ. The effectiveness of 1,064-nm long-pulsed Nd:YAG laser in the treatment of severe onychomycosis. J Cosmet Laser Ther 2016;18:317-322
Crossref
Google Scholar
PubMed
6. Karsai S, Jäger M, Oesterhelt A, Weiss C, Schneider SW, Jünger M, et al. Treating onychomycosis with the short¬pulsed 1,064-nm-Nd:YAG laser: results of a prospective randomized controlled trial. J Eur Acad Dermatol Venereol 2017;31:175-180
Crossref
Google Scholar
7. Gupta AK, Versteeg SG. A critical review of improvement rates for laser therapy used to treat toenail onychomycosis. J Eur Acad Dermatol Venereol 2017;31:1111-1118
Crossref
Google Scholar
8. Gupta AK, Foley KA, Daigle D. Clinical trials of lasers for toenail onychomycosis: The implications of new regulatory guidance. J Dermatolog Treat 2017;28:264-270
Crossref
Google Scholar
9. Ameen M, Lear JT, Madan V, Mohd Mustapa MF, Richardson M. British Association of Dermatologists' guidelines for the management of onychomycosis 2014. Br J Dermatol 2014;171:937-958
Crossref
PubMed
10. Bonhert K, Dorizas A, Sadick NS. Efficacy of combination therapy with efinaconazole 10% solution and 1,064 nm Nd:YAG laser for treatment of toenail onychomycosis. J Cosmet Laser Ther 2018;27:1-5
Crossref
Google Scholar
PubMed
11. Park KY, Suh JH, Kim BJ, Kim MN, Hong CK. Randomized clinical trial to evaluate the efficacy and safety of combination therapy with short-pulsed 1,064-nm neodymium¬doped yttrium aluminium garnet laser and amorolfine nail lacquer for onychomycosis. Ann Dermatol 2017;29:699 -705
Crossref
Google Scholar
12. Carney C, Tosti A, Daniel R, Scher R, Rich P, DeCoster J, et al. A new classification system for grading the severity of onychomycosis: Onychomycosis Severity Index. Arch Dermatol 2011;147:1277-1282
Crossref
Google Scholar
13. Kimura U, Takeuchi K, Kinoshita A, Takamori K, Hiruma M, Suga Y. Treating onychomycoses of the toenail: clinical efficacy of the sub-millisecond 1,064 nm Nd:YAG laser using a 5 mm spot diameter. J Drugs Dermatol 2012;11: 496-504
Crossref
Google Scholar
14. Shin MK, Kim TI, Kim WS, Park HK, Kim KS. Changes in nail keratin observed by Raman spectroscopy after Nd: YAG laser treatment. Microsc Res Tech 2017;80:338-343
Crossref
Google Scholar
PubMed
15. Pollak RA, Ilie C. Long-term follow-up of onychomycosis patients treated with efinaconazole. J Drugs Dermatol 2017;16:1269-1273
Crossref
Google Scholar
PubMed
16. Elewski BE, Rich P, Pollak R, Pariser DM, Watanabe S, Senda H, et al. Efinaconazole 10% solution in the treatment of toenail onychomycosis: Two phase III multicenter, randomized, double-blind studies. J Am Acad Dermatol 2013;68:600-608
Crossref
Google Scholar
17. Xu Y, Miao X, Zhou B, Luo D. Combined oral terbinafine and long-pulsed 1,064-nm Nd:YAG laser treatment is more effective for onychomycosis than either treatment alone. Dermatol Surg 2014;40:1201-1207
Crossref
Google Scholar
PubMed
18. El-Domyati M, Abdel-Wahab H, Abdel-Azim E. Nail changes and disorders in elderly Egyptians. J Cosmet Dermatol 2014;13:269-276
Crossref
Google Scholar
PubMed
Congratulatory MessageClick here!
