pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed
pISSN : 3058-423X eISSN: 3058-4302
Open Access, Peer-reviewed

Ji Hyun Lee,Hyun Ji Lee,Kyung Do Han,Hyun Min Seo,Chul Hwan Bang,Jun Young Lee,Young Min Park
10.17966/JMI.2018.23.3.63 Epub 2018 September 28
Abstract
Background: Onychomycosis is a common fungal infection of the toenails and fingernails. Although onychomycosis is a common health concern, there is a lack of nationwide studies of this condition in Korea.
Objective: We aimed to investigate the prevalence of onychomycosis according to age, month of hospital visit, and residence using national statistics provided by the National Health Insurance Service (NHIS) of South Korea in 2015.
Methods: We utilized data from the NHIS database that was procured between January and December, 2015. Statistical analyses were performed using the SAS version 9.4 (SAS Institute, Cary, NC, USA).
Results: The prevalence of onychomycosis was 3.49%. Its prevalence among individuals in their 60s (OR 5.148, 95%CI of 5.113~5.183) and 70s (OR 5.466, 95%CI of 5.427~5.505) was significantly higher than that of those in their 20s (reference age group). The highest prevalence of onychomycosis was observed in summer. The age-standardized prevalence ranged from 3.24% to 4.29% based on the place of residence, with the highest prevalence observed in provinces and large cities at lower latitudes, including Jeollanam-do, Gyeongsangnam-do, Ulsan, and Jeju-do.
Conclusion: This is the first nationwide study exploring the prevalence of onychomycosis in Korea according to the place of residence. The prevalence of onychomycosis primarily depends on age and region.
Keywords
Epidemiology Korea National health insurance Onychomycosis
Onychomycosis is a common fungal infection of the nail, representing up to 50% of all nail diseases1. This infection may be caused by dermatophytes, yeast, or non-dermatophyte molds. However, Trichophyton rubrum is the primary causative pathogen2. Fungal cutaneous infection is a major skin disease, causing troublesome health problems3. Risk factors include old age, immunocompromized condition, diabetes mellitus, polyneuropathy, peripheral arterial disease, chronic venous insufficiency, tinea pedis, and trauma4. Hyperhidrosis, occlusive shoes, and participation in sports may also be the predisposing factors5. Onychomycosis may result in severe complications in patients with diabetes6.
Previous studies have demonstrated all-type fungal infections, total cutaneous fungal infections, or subtypes of fungal species in patients with onychomycosis. Cutaneous fungal infections account for 10~20% of all dermatologic outpatient cases reported in Korea7. In 2010, the prevalence of cutaneous fungal infection was 6.51% for dermatophytosis and 0.31% for other superficial mycoses8. Yoon et al. reported that the prevalence of all-type fungal infections among the Korean population was approximately 7.1%9.
Currently, there is a lack of nationwide studies exploring the prevalence of onychomycosis in Korea. Thus, in this population-based study, we have analyzed the prevalence of onychomycosis using data obtained from the Korean National Health Insurance Service (NHIS) in 2015.
1. Data source
We utilized data from the NHIS database obtained between January and December, 2015. The Korean NHIS monitors all medical services in Korea; 100% of the Korean population is covered under the NHIS. This computerized database includes all claim data, such as patient demographics, dates of hospital visits, residence, socioeconomic status, and claimed treatment details based on the International Classification of Disease (ICD)-10 codes10.
2. Study sample
We analyzed data for patients who visited clinics or hospitals with a diagnostic code (ICD-10) of onychomycosis (Tinea ungium) (B351) more than once between January and December, 2015. Patients with other types of dermatophytosis, including Tinea pedis and those with missing data, were excluded from the analysis. This study was approved by the institutional review boards of the Korean National Institute for Bioethics Policy (NHIS-2017-1-002), the Korea Centers for Disease Control and Prevention, and the Catholic University of Korea (No. KC16EISE0923).
3. Study variables
NHIS data were interpreted to calculate the national prevalence of onychomycosis in each city or province of Korea. Patients were classified into nine age groups as follows: 0~9, 10~19, 20~29, 30~39, 40~49, 50~59, 60~69, 70~79, and >80 years. The region of residence for each patient was defined as urban (Seoul, Busan, Daegu, Incheon, Gwangju, Daejeon, Ulsan, Sejong, and Gyeonggi-do) or rural (Gangwon-do, Chungcheongbuk-do, Chungcheongnam-do, Jeollabuk-do, Jeollanam-do, Gyeongsangbuk-do, Gyeongsangnam-do, and Jeju-do)11. Further, assessment of the influence of the month of hospital visit on the prevalence of onychomycosis was also performed.
4. Statistical analysis
Statistical analyses were performed using the SAS version 9.4 (SAS Institute, Cary, NC, USA) statistical software. Age-specific rates of prevalence of onychomycosis were calculated by dividing the number of patients with onychomycosis by the total Korean population according to the 2010 Population and Housing Census. p-values < 0.05 were considered statistically significant.
1. Characteristics of patients with onycho- mycosis
In 2015, total 1,917,588 patients with onychomycosis were covered under the NHIS and the prevalence of onychomycosis was 3.49%. The prevalence of onychomycosis tended to in- crease with age (Table 1). The prevalence of onychomycosis among patients aged 60~69 years [odds ratio (OR) 5.148, 95% confidence interval (CI) 5.113~5.183)] and 70~79 years (OR 5.466, 95% CI 5.427~5.505) were significantly higher than that reported in patients aged 20~29 years (reference age group). In addition, the prevalence of onychomycosis was higher in females than in males across all age groups. The prevalence was 3.59% for males and 3.84% for females. Females aged 70~79 years had the highest prevalence of onychomycosis (OR 6.597, 95% CI 6.527~6.668). However, the prevalence of onychomycosis among patients aged 0~9 and 10~19 years was 0.088 (0.086~0.090) and 0.405 (0.401~ 0.410), respectively, which is lower than that reported in the reference group.
|
Age |
Total |
Male |
Female |
||||||
|
Reference |
Onychomycosis |
OR |
Reference population |
Onychomycosis |
OR |
Reference population |
Onychomycosis |
OR |
|
|
0~9 |
4,605,930 |
6,761 |
0.088 |
2,370,685 |
368 |
0.083 |
2,235,245 |
2,993 |
0.095 |
|
10~19 |
5,980,471 |
40,217 |
0.405 |
3,126,473 |
23,667 |
0.400 |
2,853,998 |
16,550 |
0.414 |
|
20~29 |
6,821,889 |
112,087 |
-ref- |
3,602,702 |
67,410 |
-ref- |
3,219,187 |
44,677 |
-ref- |
|
30~39 |
7,945,906 |
211,874 |
1.640 |
4,074,241 |
120,676 |
1.601 |
3,871,665 |
91,198 |
1.714 |
|
40~49 |
8,934,467 |
358,249 |
2.501 |
4,535,856 |
176,283 |
2.121 |
4,398,611 |
181,966 |
3.066 |
|
50~59 |
8,210,181 |
488,090 |
3.784 |
4,121,285 |
227,600 |
3.066 |
4,088,896 |
260,490 |
4.835 |
|
60~69 |
4,691,566 |
371,495 |
5.148 |
2,276,167 |
174,038 |
4.342 |
2,415,399 |
197,457 |
6.326 |
|
70~79 |
3,124,667 |
261,451 |
5.466 |
1,327,943 |
108,812 |
4.681 |
1,796,724 |
152,639 |
6.597 |
|
≥80 |
1,258,967 |
64,047 |
3.209 |
378,167 |
23,941 |
3.545 |
880,800 |
40,106 |
3.390 |
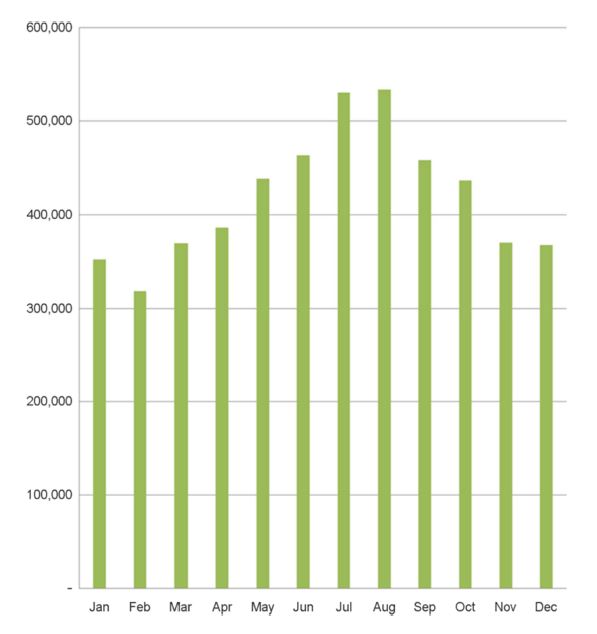
2. Monthly prevalence
The highest prevalence of onychomycosis was observed in July and August. The lowest prevalence of onychomycosis was noted in January and February (Figure 1).
3. Place of residence
When the age-standardized prevalence was calculated using the 2010 Census Korean population, Jeollanam-do (4.29%), Gyeongsangnam-do (3.99%), Ulsan (3.89%), and Jeju-do (3.88%) showed a much higher prevalence of onychomycosis than other areas. Conversely, the age-standardized prevalence in Seoul (3.24%) and Gyeonggi-do (3.31%) was relatively low (Figure 2).

This was the first large-scale population-based study, evaluating the epidemiology of onychomycosis in Korea. The prevalence of onychomycosis was shown to be dependent on age and region.
The impact of age on the prevalence of onychomycosis in a population is very important. There is a positive correlation between onychomycosis prevalence and age12. In the current study, the prevalence of onychomycosis increased with age, i.e., the highest prevalence was observed in patients aged 60~69 and 70~79 years. Advanced age is considered a risk factor of onychomycosis owing to diminished blood circulation, longer exposure to fungi, slower growth of nails and nail thickening, and increased susceptibility to infection.
We observed a female predominance in the prevalence of onychomycosis. This finding was consistent with that of a previous study in Spain showing that the prevalence of onychomycosis among females was higher than that reported in males (1.8% vs. 0.8%, respectively)13. However, other studies have demonstrated that onychomycosis is more prevalent in males than in males14-17. In the United Kingdom, a population survey showed a prevalence of dermatophyte nail infection of 2.8% in males and 2.6% in females14. In Finland, the prevalence of onychomycosis identified as dermatophyte culture-positive cases was 13% in males and 4.3% in females15. In Iceland, based on photograph evaluations by patients, 195 males (17.5%) and 187 females (13.7%) identified themselves as having onychomycotic nails16. In another study in Spain, the prevalence of onychomycosis was 3.1% (CI 95% 2.12~4.38), 4.4% (CI 95% 2.7~6.7), and 1.9% (CI 95% 0.9~ 3.4), in total, males, and females, respectively17. The discrepancies among the results of studies may be explained by the finding that Korean females are more likely to seek medical attention than Korean males. Another possible explanation is that susceptibility to such infections varies between ethnic groups.
Moreover, the results of the current study suggest that the prevalence of onychomycosis in Korea is related to environmental factors. Firstly, we observed seasonal differences in the month of hospital visit among the studied groups. Secondly, we observed regional differences in the prevalence of onychomycosis, with higher prevalence reported in lower latitudes, such as Jeollanam-do, Gyeongsangnam-do, Ulsan, and Jeju-do. Although the reason for this regional difference remains unclear, we hypothesize that environmental factors such as high temperature and humidity may play key roles. These factors may increase sweating and provoke the development of onychomycosis.
The limitations of this study must be acknowledged. Firstly, access to medical care differs from region to region. Secondly, we did not make mycologic diagnoses using potassium hydroxide or fungus culture. Despite these limitations, this was the first nationally representative, population-based study, evaluating patients with onychomycosis in Korea.
The results of the current study suggest that onychomycosis is most prevalent in elderly patients living at lower latitudes. This high prevalence may be because of the hot, humid weather in such provinces in South Korea.
In relation to this article, I declare that there is no conflict of interest.
References
1. Summerbell RC, Kane J, Krajden S. Onychomycosis, tinea pedis and tinea manuum caused by non-dermatophytic filamentous fungi. Mycoses 1989;32:609-619
Crossref
Google Scholar
2. Foster KW, Ghannoum MA, Elewski BE. Epidemiologic surveillance of cutaneous fungal infection in the United States from 1999 to 2002. J Am Acad Dermatol 2004; 50:748-752
Crossref
Google Scholar
3. Hay RJ, Fuller LC. Global burden of skin disease in the elderly: a grand challenge to skin health. G Ital Dermatol Venereol 2015;150:693-698
Crossref
Google Scholar
PubMed
4. Ghannoum MA, Hajjeh RA, Scher R, Konnikov N, Gupta AK, Summerbell R, et al. A large-scale North American study of fungal isolates from nails: the frequency of onychomycosis, fungal distribution, and antifungal suscepti- bility patterns. J Am Acad Dermatol 2000;43:641-648
Crossref
Google Scholar
5. Papini M, Piraccini BM, Difonzo E, Brunoro A. Epidemiology of onychomycosis in Italy: prevalence data and risk factor identification. Mycoses 2015;58:659-664
Crossref
Google Scholar
PubMed
6. Rich P, Hare A. Onychomycosis in a special patient population: focus on the diabetic. Int J Dermatol 1999;38 Suppl 2:17-19
Crossref
Google Scholar
PubMed
7. Suh SB. Dermatophytosis and its causative agents in Korea. Korean J Med Mycol 1999;1:1-10
Crossref
Google Scholar
8. Kim SH, Cho SH, Youn SK, Park JS, Choi JT, Bak YS, et al. Epidemiological characterization of skin fungal infections between the years 2006 and 2010 in Korea. Osong Public Health Res Perspect 2015;6:341-345
Crossref
Google Scholar
9. Yoon HJ, Choi HY, Kim YK, Song YJ, Ki M. Prevalence of fungal infections using National Health Insurance data from 2009-2013, South Korea. Epidemiol Health 2014; 36:e2014017
Crossref
Google Scholar
10. Koo BK, Lee CH, Yang BR, Hwang SS, Choi NK. The incidence and prevalence of diabetes mellitus and related atherosclerotic complications in Korea: a National Health Insurance Database Study. PLoS One 2014;9:e110650
Crossref
Google Scholar
11. Lee JH, Han KD, Kim KM, Park YG, Lee JY, Park YM. Prevalence of Atopic Dermatitis in Korean Children Based on Data From the 2008-2011 Korean National Health and Nutrition Examination Survey. Allergy Asthma Immunol Res 2016;8:79-83
Crossref
Google Scholar
12. Gupta AK, Daigle D, Foley KA. The prevalence of culture-confirmed toenail onychomycosis in at-risk patient populations. J Eur Acad Dermatol Venereol 2015;29:1039 -1044
Crossref
Google Scholar
13. Sais G, Jucgla A, Peyri J. Prevalence of dermatophyte onychomycosis in Spain: a cross-sectional study. Br J Dermatol 1995;132:758-761
Crossref
Google Scholar
PubMed
14. Roberts DT. Prevalence of dermatophyte onychomycosis in the United Kingdom: results of an omnibus survey. Br J Dermatol 1992;126 Suppl 39:23-27
Crossref
Google Scholar
15. Heikkila H, Stubb S. The prevalence of onychomycosis in Finland. Br J Dermatol 1995;133:699-703
Crossref
Google Scholar
PubMed
16. Sigurgeirsson B, Steingrimsson O, Sveinsdottir S. Prevalence of onychomycosis in Iceland: a population-based study. Acta Derm Venereol 2002;82:467-469
Crossref
Google Scholar
PubMed
17. del Palacio A, Cuetara MS, Garau M, Perea S. Onychomycosis: a prospective survey of prevalence and etiology in Madrid. Int J Dermatol 2006;45:874-876
Crossref
Google Scholar
PubMed
Congratulatory MessageClick here!
